Squamous cell
carcinoma, a rare variant of primary breast carcinoma: a case report
Kapil Rampal 1, Parampreet
Singh 1*, Harkanwalpreet Kaur 1,
Meghna Sharma 2, Rajvir Kaur 1
1 Ggsmch, Faridkot, Punjab, India
2 Gmc,
Amritsar, Punjab, India
Corresponding Authors: Parampreet
Singh
* Email: param18192@gmail.com
Abstract
Introduction: Breast cancer is the most common malignancy occurring worldwide in
females but primary squamous cell carcinoma represents a very rare variant of
breast carcinoma, accounting for less than 0.1%. Mostly it is grayish-white in colour with an ill-defined cut surface and has cystic areas
of foci of necrosis macroscopically. Squamous elements in these neoplasms can
range from well to poorly differentiated. The majority was moderately
differentiated and showed cystic degeneration correlating with the macroscopic
appearance.
Case presentation: A 45-year-old female
presented to us with a painless progressive lump involving all quadrants of
left breast that at presentation had involved the whole breast and was
associated with foul-smelling discharge. The patient had toxic features and was
taken up for toilet mastectomy. The wound was left open for a delayed closure.
The histopathological report suggested triple negative squamous cell carcinoma
involving the breast.
Discussion: Squamous cell carcinoma is commonly seen in the skin and lung, it rarely originates in breast tissue. There are
reports that it may develop within a previous benign lesion such as an
epidermal cyst or chronic inflammatory lesions. It may also mimic benign breast
disease resulting in inappropriate or delayed management. Clinically and radiologically it is indistinguishable from adenocarcinoma,
the most common presentation being cystic lesion. Because of limited data and
few case reports worldwide, management strategies have been controversial.
Total mastectomy with axillary clearance is usually done. As it is locally
advanced, conservative surgery is not feasible most of the time. Radiotherapy
has been used in locally advanced cases, though not much useful.
Conclusion: This case report highlights the rare occurrence of synchronous primary
malignancies in the lung and breast, underreported in the medical literature.
This case adds to the existing knowledge of MPMT and may stimulate further
research on this topic. Clinicians should be aware of the possibility of MPMT
in cancer patients and perform thorough investigations to rule out secondary or
metastatic tumors.
Keywords: Small cell carcinoma, Breast cancer, Synchronous, Metachronous,
Histopathology, Immunochemistry, Gene mutation
Introduction
Breast cancer is the most common malignancy occurring
worldwide in females but primary squamous cell carcinoma represents a very rare
variant of breast carcinoma, accounting for less than 0.1% (1). It is a highly
aggressive tumor with a greater tendency to metastasize
as compared to adenocarcinoma breast, thus having a poor prognosis. The lesions
are usually larger, hormone receptor-negative with lesser nodal spread. Apart
from adenocarcinoma breast, it needs to be differentiated from primary squamous
cell carcinoma of skin overlying breast and metastatic squamous cell carcinoma
from some distant site. As clinical and radiological findings are not specific,
the biopsy is a must to diagnose this variant. For diagnosis of squamous cell
carcinoma, more than 90% of cells should be squamous (2).Murcia
and colleague defined pure squamous cell carcinoma as:
1) No other neoplastic component such as ductal or
mesenchymal element is present in tumour.
2) Tumor origin must be
independent from the overlying skin and nipple.
3) Absence of an associated primary squamous cell
carcinoma in a second site (3).
Pathogenesis
Gross Findings
Mostly it is grayish white
with an ill-defined cut surface and has cystic areas of foci of necrosis
macroscopically. A wide range of sizes was reported, often larger than other
special types (4).
Microscopic Findings
Squamous elements in these neoplasms can range from
well to poorly differentiated. The majority was moderately differentiated and showed
cystic degeneration (resembling cutaneous inclusion cyst) correlating with the
macroscopic appearance. A small (<25%) spindle cell component may be
present. Spindled components may range from low to high grade. In some cases associated DCIS confirms the primary nature of the
lesion (4,5).
Immunohistochemistry
Estrogen receptor (ER) assays have been variable and no reliable conclusion can
be drawn and mostly regarded as ER negative. Focally tumor
express cytokeratins; shows immunostaining for S100
and smooth muscle actin (4).
We report a
case of this rare variant of breast carcinoma along with the management done.
Case presentation
45 year old female presented to us with a painless progressive lump involving all
quadrants of the left breast that at presentation had involved the whole breast
and was associated with foul-smelling discharge (Figure 1).

Figure 1. Gross image of breast mass.
The patient had toxic features and was taken up for
toilet mastectomy. The wound was left open for a delayed closure. The
histopathological report suggested triple negative squamous cell carcinoma
involving the breast. (Figure 2).
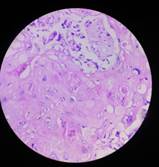
Figure 2. HP image of SCC.
Discussion
Squamous cell carcinoma is commonly seen in the skin
and lungs, it rarely originates in breast tissue. Although its origin is
unclear, multiple hypotheses have been proposed. Murialdo
R et al(6). state that it originates from the epithelium
of the mammary ducts or squamous metaplasia of adenocarcinoma. There are
reports that it may develop within a previous benign lesion such as an epidermal
cyst or chronic inflammatory lesions (7). It may also mimic benign breast
disease resulting in inappropriate or delayed management (7).
Clinically and radiologically
it is indistinguishable from adenocarcinoma, the most common presentation being
a cystic lesion. The typical presentation is a hard breast lump, which may have
inflammatory signs in an elderly woman. Although it is larger, the tendency for
nodal spread is lesser than adenocarcinoma as stated by Vekariya
M et al (1). and Carbone S et al (8). 70% of squamous cell carcinoma of the breast
don’t have axillary lymphadenopathy at presentation but lymph node dissection
could always be performed for staging due to unpredictable lymph node
dissemination. Distant metastasis is comparatively higher. Hormone receptor
(ER/PR) and HER2/neu- are usually negative with overexpression of EGFR.
Because of limited data and few case reports
worldwide, management strategies have been controversial. Total mastectomy with
axillary clearance is usually done. As it is locally advanced, conservative
surgery is not feasible most of the time. Radiotherapy has been used in locally
advanced cases, though not very useful. They are reported to be resistant to
standard chemotherapy used for adenocarcinoma, as well as hormonal therapy.
Several chemotherapeutic agents have been tried to date but efficacy and response
have not been estimated yet. Hennessy et al (9) reported no benefit in using anthracycline/taxane-based neoadjuvant chemotherapy. In contrast, few
have also reported a good response with neoadjuvant therapy using cisplatin and
5-fluoro-uracil (10). A high incidence of recurrence had been reported in those
who received adjuvant chemotherapy (11). Due to the high rates of locoregional
recurrence in this disease, early adjuvant radiation therapy is thought to be
prudent despite reports of frequent recurrence in irradiated fields. Adjuvant
chemotherapy is used regularly given the aggressive nature, but the risk of
distant metastasis remains high in SCC (12,13). Historically,
anthracycline-containing regimens have been the standard; however, the use of
carboplatin and taxanes has biological plausibility
and have been employed.
Conclusion
Very rare incidence along with nonspecific
presentation poses a major challenge in the diagnosis of primary SCC.
Subsequent challenges being variable responses or resistance to standard
chemotherapy regimens as well as hormonal agents. EGFR positivity had been a
scope for targeting specific chemotherapeutic agents.
Author contribution
PS supervised and
corresponding author, KR, HK, and
MS contributed to some parts of the study and RK contributed as an
anesthetist.
Conflict of interest
The
authors declare no conflict of interest.
References
1. Vekariya M, Gupta V, Pednekar A, Nagur B, Mahna A et al.
Primary squamous cell carcinoma of the breast: A rare case report. Int J Sci
Stud 2014;2(8):226-228.
2. Kamra H,
Gadgil P, Chaware S, Kanade U. Acantholytic variant of squamous cell carcinoma
of breast: a rare case report. Ecancermedicalscience.
2011;5:214.
3. Macia M, Ces JA, Becerra E, Novo A. Pure squamous carcinoma of the
breast. Report of a case diagnosed by aspiration cytology. Acta Cytol. 1989
Mar-Apr;33(2):201-4.
4. O’Malley FP,
Pinder SE, Mulligan AN. In: Breast pathology: a volume in the series:
foundation in diagnostic pathogy. 2nd ed. Elsevier:
United states 2011.p.216.
5. Gobbi H,
Simpson JF, Borowsky A, Jensen RA, Page DL. Metaplastic breast tumors with a
dominant fibromatosis-like phenotype have a high risk of local recurrence.
Cancer. 1999 May 15;85(10):2170-82.
6. Murialdo R, Boy D, Musizzano Y,
Tixi L, Murelli F et al. Squamous cell carcinoma of the breast: a case report.
Cases J. 2009 Jul 10;2:7336.
7. Flikweert, E.R., Hofstee, M. & Liem, M.S. Squamous cell
carcinoma of the breast: a case report. World J Surg Onc
6, 135 (2008).
8. Carbone S,
Lobo Alvarez R, Lamacchia A, Almenar Gil A, Martin Hernandez R et al. Primary
squamous cell carcinoma of the breast: A rare case report. Rep Pract Oncol Radiother. 2012 Aug
9;17(6):363-6.
9. Hennessy BT,
Krishnamurthy S, Giordano S, Buchholz TA, Kau SW et al. Squamous cell carcinoma
of the breast. J Clin Oncol. 2005 Nov 1;23(31):7827-35.
10. Seddik Y,
Brahmi SA, Afqir S. Primary squamous cell carcinoma
of the breast: a case report and review of literature. Pan Afr
Med J. 2015 Feb 18;20:152.
11 . Pandey A,
Joshi K, Moussouris H, Joseph G. Case Reports on
Metaplastic Squamous Cell Carcinoma of the Breast and Treatment Dilemma. Case
Rep Oncol Med. 2019 Sep 18;2019:4307281.
12. Hennessy BT, Krishnamurthy S, Giordano S, Buchholz TA, Kau SW, Duan Z.
Squamous cell carcinoma of the breast. J Clin Oncol. 2005 Nov
1;23(31):7827-7835.
13. Behranwala KA, Nasiri N, Abdullah N,
et al. Squamous cell carcinoma of the breast: Clinico-pathologic
implications and outcome. Eur J Surg
Oncol. 29:386,2003-389