Isolated intraperitoneal urinary
bladder rupture following blunt trauma abdomen: a case study
Parampreet Singh Sandhu
Param 1*, Amandeep Singh 1, Ashutosh Talwar 1,
Haramritpal Kaur 1, Robinpreet
Kaur 1, Rupali Sehgal 1, Rajvir Kaur 2
1 Department of General Surgery, Guru Gobind Singh Medical College
and Hospital Faridkot, Punjab, India
2 Department of Anesthesiology, Guru Gobind Singh Medical College and
Hospital Faridkot, Punjab, India
Corresponding
Authors: Parampreet Singh Sandhu Param
* Email: param18192@gmail.com
Abstract
Introduction: Urinary bladder injuries present in emergencies in the set up of road traffic accidents with blunt trauma to the abdomen.
Bladder injury can be extraperitoneal, intraperitoneal, or mixed.
Intraperitoneal bladder ruptures comprise 15% of all bladder injuries. The most
common feature of bladder rupture is hematuria, which can be either microscopic
or gross. We hereby present a case of isolated urinary bladder intraperitoneal
rupture following a roadside accident due to its rarity.
Case presentation: The 29-year-old male was brought to emergency with an alleged history
of Roadside accidents with a distended abdomen. Hematuria is present on Foley’s
catheterization. X-ray of the pelvis was normal. Contrast-enhanced computerized
tomography whole abdomen showed bladder rupture. The patient was taken up for
exploratory laparotomy and bladder repair. The postoperative period was
uneventful.
Discussion: In blunt abdominal trauma, up to 90% of bladder injuries are often
associated with pelvic fractures. Isolated traumatic bladder rupture is rare.
In intraperitoneal bladder rupture, urine gets collected in the peritoneal
cavity. Intraperitoneal bladder rupture requires exploratory laparotomy and the
site of rupture is treated by suturing the bladder in two layers with
absorbable sutures. Postoperative care is focused on preventing urinary catheter-associated
infections.
Conclusion: This case report highlights the rare occurrence of isolated bladder
rupture in cases of Road traffic accidents. Our patient recovered uneventfully
after exploratory laparotomy and surgical repair.
Keywords: Urinary bladder, Rupture, Extraperitoneal, Intraperitoneal, Trauma
Introduction
Urinary
bladder injuries present in an emergency in the set up
of road traffic accidents with blunt trauma to the abdomen. Relatively uncommon
these days, patients with bladder injury comprise 0.36% of all blunt trauma
abdomen patients (1). Bladder injuries occur as a result of a direct blow to
the distended bladder. These patients have classical symptoms of suprapubic
pain with gross hematuria. Signs of peritonism like tenderness, guarding, and rigidity
can be seen on examination in a few cases (2).
Bladder
injury can be extraperitoneal, intraperitoneal, or mixed. Extraperitoneal
bladder injury is most common and is associated with pelvic fracture and occurs
as a result of decelerating injuries. These mostly involve the anterolateral
wall, trigone, or neck of the urinary bladder. In these cases, urine
extravasation is extraperitoneal and confined around the bladder. Thus, FAST (Focused
assessment with sonography for trauma) stays negative in these injuries. Most
of these cases can be managed conservatively barring a few complex
extraperitoneal bladder ruptures (3).
Intraperitoneal
bladder ruptures comprise 15% of all bladder injuries. It is more prone to
occur at the dome of the bladder since this wall is mobile. Urine extravasates
into the abdomen and so, FAST is positive. Surgical repair of these injuries is
crucial with 100% success rate in most cases (4,5).
We
present a rare case of isolated urinary bladder intraperitoneal rupture
following a roadside accident due to its rarity.
Case presentation
A 29-year-old male was brought to the emergency
department, GGSMCH, Faridkot after a roadside accident in which a patient was
driving his bike and got hit by a tractor. As narrated by the patient himself,
just after the collision, he lost his balance and fell, hitting his lower
abdomen over the bike’s handle. He also states that he felt the urge to void
urine before the accident but neglected it. The patient did not experience any
head trauma. He was brought in an ambulance to the emergency department. The
patient had tachycardia of 110 beats per minute with a normal blood pressure of
110/76 mm of mercury. GCS was 15/15.
On
examination, the abdomen was distended and guarding was present in the lower
abdomen. No blood was present at the tip of the meatus. Upon catheterization of
the urinary bladder, blood-mixed urine was drained. The patient was
resuscitated with IV fluids, IV antibiotics, IV analgesics, and hemostatic
agents. He had no known comorbidities.
X-Ray pelvis
ruled out any pelvic fracture as depicted in Figure 1. The patient's blood
workup revealed hemoglobin: 17, TLC counts: of 11.3 and Serum Creatinine of 1.3.

Figure 1. X-ray pelvis showing no obvious bony
injury.
Ultrasonography whole abdomen revealed free fluid
with internal echoes in the pelvis. CECT abdomen(being
the investigation of choice for blunt trauma abdomen) revealed gross spillage
of dye from the bladder into the peritoneum suggestive of intraperitoneal
bladder rupture as depicted in figure 2 (arrowhead). No other visceral injury
was seen. Gross free fluid was noted in the peritoneum.
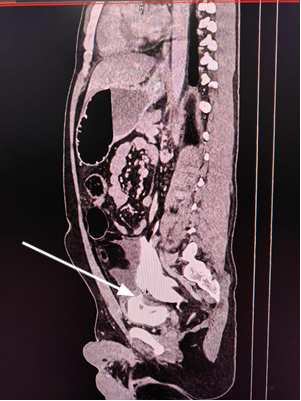
Figure 2. CECT whole abdomen with pelvis showing
contrast extravasation from the bladder into the peritoneal cavity.
The patient was taken up for exploratory laparotomy
and the following findings were reported: 1L blood mixed urine along with blood
clots drained from the peritoneal cavity; intraperitoneal urinary bladder
rupture full thickness through the dome of the urinary bladder(as
depicted in figure 3; All the solid and hollow viscera were found to be normal.
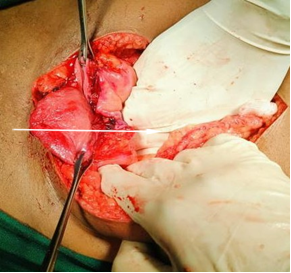
Figure 3. Intraoperative photograph showing ruptured
bladder dome.
The bladder was repaired in a double layer using Vicryl 3-0 round body sutures. The abdomen was closed in
layers. Pelvic drain left in situ. Three A suprapubic catheter was left in situ.
The patient was monitored closely postoperatively.
Vital monitoring along with daily urine output charting in the suprapubic
catheter and the per urethral catheter was done. The patient’s post-operative
period remained uneventful with no distension or any other fresh complaints. The
patient was discharged in satisfactory condition after 7 days with the suprapubic
catheter in situ. The patient was followed up for 6 weeks. The suprapubic
catheter was removed on POD 21 following the cystourethrogram, which was found
to be normal. The patient had a follow up for 4 weeks with no fresh complaints.
Discussion
bladder;
or high-energy abdominal trauma, which can lead to pelvic fracture and bladder
injuries; or penetrating and iatrogenic injuries, frequently with a motor
vehicle accident (MVA) (6).
In
blunt abdominal trauma, up to 90% of bladder injuries are often associated with
pelvic fractures. Isolated traumatic bladder rupture is rare, but
extraperitoneal rupture is frequent, accounting for 80% of the cases (7). A
blow to the lower abdomen in a patient with a distended bladder may result in the
rupture of the weakest part of the bladder due to the increased intravesical
pressure. The bladder dome is in contact with the peritoneal surface and is a
weak point that is susceptible to rupture.
The
most common feature of bladder rupture is hematuria, either microscopic or
gross hematuria and intraperitoneal bladder rupture results in urine getting
collected in the peritoneal cavity resulting in the signs of peritonitis.
Hematuria is absent in 15% of cases of intraperitoneal bladder rupture. Delayed
presentation is seen in some cases with non-passage of urine and lower
abdominal pain. Intraperitoneal rupture of the bladder leads to urinary
ascites. This leads to an increase in the levels of serum urea, creatinine and
Potassium with the decrease in serum sodium concentration.
Ultrasonography
is a very widespread diagnostic method, but has a limited role. The
investigation of choice is CECT Whole abdomen with pelvis.
Non-operative
management can occasionally be applied for extraperitoneal bladder rupture but
intraperitoneal rupture of the bladder must be explored surgically
Intraperitoneal bladder rupture requires exploratory laparotomy and the site of
rupture is treated by suturing the bladder in two layers with absorbable
suture. Permanent sutures represent a potential nidus for calcium deposition
and future bladder stone formation (8).
In
our patient abdomen was distended with generalized tenderness and guarding
along with gross hematuria was present on catheterization.CECT's
whole abdomen revealed rupture of the bladder dome along with extravasation of
contrast into the peritoneal cavity. So, the patient was immediately taken up
for exploratory laparotomy, and bladder repair was done.
Conclusion
This case report highlights the rare occurrence of
isolated bladder rupture in cases of Road traffic accidents. Careful attitude
and thorough knowledge about the mechanism of injury is the cornerstone for
proper diagnosis and early management of the patient.
Author
contribution
PSSP, AS, and
AT wrote the manuscript, RoK, and RS prepared figures, and
HK, RaK proofread.
Patients
consent
The
patient’s informed consent was taken for academic purposes.
Conflict
of interest
There
are no Conflicts of interest.
Funding
There
is no funding.
References
Matlock K.A, Tyroch A.H, Kronfol Z.N, McLean S.F, Pirela-Cruz M.A. Blunt Traumatic
bladder rupture: a 10-year perspective, Am. Surg. 79 (2013) 589–93.
2. Guttmann .I, Kerr H.A,
Blunt bladder injury, Clin. Sports Med. 32 (2013) 239–46.
3.Elkbuli A, Ehrhardt JD, Hai S, McKenney M, Boneva D
Management of blunt intraperitoneal bladder rupture: case report and literature
review. Int J Surg 2019;55:160–3.
4. Corriere J.N.Jr,
Sandler C.M. Management of the ruptured bladder: J. Trauma .1986 830–33.
5. Inaba K, McKenney M, Munera F, Cystogram follow-up
in the Management of traumatic bladder disruption, J Trauma;(2006) 23–8.
6.Detanac D, Filipovic N, Sengul I, Zecovic E, Muratovic S, Sengul D. Extraordinarily Rare
Isolated Intraperitoneal Urinary Bladder Rupture in Blunt Abdominal Injury
Without Pelvic Fracture: An Aide-Mémoire. Cureus.
2022 ;14(8)
7.Grünherz L, Startseva X, Kozomara-Hocke M, Barth BK, Simmen HP, Mica L et al.Combined intraand
extraperitoneal urinary bladder rupture – a rare seat-belt injury. Int J Surg Case Rep. 2017;38:119–21.
8.Jang H, Park E.K, Han D.S, Kim C.J, Lee Y.S. Bladder
stone formation on permanent suture material ten years after laparoscopic high
uterosacral ligament suspension:Clin.
Exp. Obstet. Gynecol., 44 (3) (2017), pp. 472-4.