Management of oligometastatic
triple-negative breast cancer with lung metastasis using 4DCT: a case report
Siddharth Arora
1*, Kriti Grover 1
1 Rohilkhand Medical College and Hospital, Bareilly, Uttar Pradesh,
India
Corresponding
Authors: Siddharth Arora
*
Email: drsiddhartharora25@gmail.com
Abstract
Introduction: Breast cancer remains the most prevalent disease in women.
Oligometastatic breast cancer (OMBC), is defined by a limited disease burden.
40% of Triple negative breast cancer are associated with Lung metastasis.
Stereotactic body radiotherapy is used for lung metastasis. We report a case of
oligometastatic triple-negative breast cancer with lung metastasis treated with
the deep inspiratory breath hold technique via four-dimensional (4D)
respiratory correlated CT imaging (4DCT).
Case presentation: A 77-year-old Asian Indian female patient presented with breathing
difficulty. Evaluation revealed it as Oligometastatic breast carcinoma with
solitary lung metastasis. She was treated with SBRT to her lung lesion using
4DCT after her primary management.
Discussion: 4DCT has revolutionized the radiotherapy planning for gated
radiotherapy delivery. Retrospective 4DCT allows the reconstruction of a number
of breathing phases that demonstrate the motion of the tumor and surrounding
tissue. Despite its limits, the addition of this technology has been beneficial
to the overall sector.
Conclusion: A total dose of 50 Gy in 5 fractions (BED10: 100 Gy) via volumetric
modulated arc therapy (VMAT) was delivered to solitary lung metastasis. During
surveillance imaging with PET/CT, there was no sign of progression or distant
failure, and the treated lesion responded almost completely after 3 months
beyond evidence of pneumonitis.
Keywords: Oligometastatic, CyberKnife, Breast cancer, Four-dimensional computed
tomography (4DCT), Lung metastasis
Introduction
Survival
of patients with metastatic breast cancer has improved. Oligometastatic breast
cancer (OMBC), is an independent prognostic factor (1, 2). The most common
definition uses up to five metastases (3). The optimal treatment for OMBC has
yet to be determined, yet systemic therapy remains key. Lung metastasis is
commonly diagnosed in TNBC. Stereotactic body radiotherapy (SBRT) is an
advancement over traditional conventional radiotherapy and is delivered in
fewer fractions. It is commonly used for lung, liver, or adrenal metastasis
(4). Respiratory motion management is useful for targets moving beyond 5 mm,
especially those in the lungs and liver. Marker blocks on the chest or abdomen
(RPM respiratory gating), have been widely used. The traditional wider gating
has been reduced to a very low gating amplitude. A tool used to measure
breathing motion is 4DCT. 4DCT is a motion-encompassing method introduced in
the early 2000s. Its goal is to depict the temporal dynamics of a 3D sample
with high temporal and spatial precision. 4DCT will often use a gating
approach, such as breathing tracking, to automatically initiate picture
acquisition at predetermined points. Additionally, the radiation beam is only
activated during specific breathing cycle points (e.g., the deep inspiration
breath-hold technique). We report a case of oligometastatic triple-negative
breast cancer with lung metastasis. The solitary lung metastasis was treated
with the deep inspiratory breath hold technique via 4DCT. The reports talk
about the 4DCT technique, its advantages over conventional free breathing
technique and 3DCRT and its disadvantages.
Case
presentation
A 77-year-old Asian Indian female patient
presented with a lump in her right breast in the
outer quadrant. On examination, an ulceroproliferative mass measuring 7.5 cm x
7.5 cm was felt in the right outer quadrant; the base and the nipple-areola
complex were uninvolved. The nipple was not retracted. A single palpable node
was felt in the right axillary region measuring 1 cm by 1 cm. Core biopsy from
the lump revealed invasive breast cancer (no special type), Nottingham grade II
(overall score of 7). The IHC-4 panel suggests that there are negative estrogen
receptors, negative progesterone receptors, and equivocal human epidermal
growth factor receptor 2 (Her2neu) with a Ki67-30--40%. Fluorescent in situ
hybridization (FISH) was negative for Her2neu. PET-CT revealed a faintly
metabolically active soft tissue nodule is seen in the posterior basal segment
of the left lung lower lobe of the left lung measuring 1.1 × 1.4 cm in addition
to the primary segment. SBRT was planned to treat her solitary metastatic
lesion in her lung with 4D CT. (Figures 1, 2).
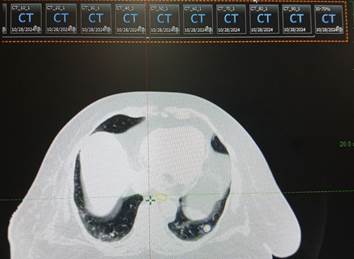
Figure 1. 4DCT acquisition - average RPM
(Respiration Per Minute) for at least 10 breathing cycles.
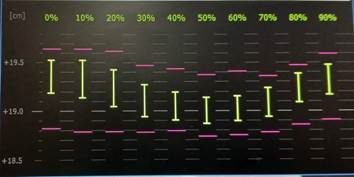
Figure 2. 4DCT waveform (showing highest Tumor
velocity and tumor stability between 30-70% phases).
Plans were calculated with 6MV FFF (Figure 3).
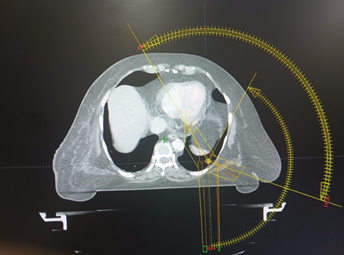
Figure 3. Arc offsets (use of 3 arcs, including a
partial arc).
Discussion
Lung
metastases have very devastating clinical presentations and consequences, in
addition to the poor prognosis associated with metastatic breast cancer.
Metastatic breast cancer to lung presents with constant cough, pain, difficulty
breathing or shortness of breath, wheezing, fatigue, recurring infections in
the chest, coughing up blood or unintentional weight loss. 5-year survival rate
as per The Surveillance, Epidemiology, and End Results (SEER) database such as
lung is 30 %. According to gene expression study, the luminal B and basal
subtypes had the highest numbers of lung recurrence patients. Despite receiving
chemotherapy, targeted therapy, and endocrine therapy based on molecular
receptor profiles, patients with lung metastases from breast cancer still have
a poor prognosis. Early diagnosis is now the best and only way to prevent lung
metastases from breast cancer. Therefore, in order to develop more effective
treatment plans, we need to completely comprehend the mechanism of breast
cancer lung metastases. According to studies, patients with low volume OMBC may
see an improvement in progression-free survival or long-term disease remission.
Since
the mid-1980s, efforts have been made to improve outcomes through escalating
radiotherapy doses. SBRT is low morbidity non-invasive option or
metastasis-directed curative intent therapy. SBRT is an advanced type of
external beam radiation therapy that uses a small number (one to five) of
high-dose fractions. SBRT is being utilized in oligometastatic disease and in
patients who have oligoprogressive disease. SBRT can also be used for patients
with limited lung metastases or limited metastases to other body sites (5).
Prospective series have shown similar overall survival and cancer-specific
survival between SBRT and lobectomy. Deep Inspiration Breath Hold (DIBH) SBRT
is an improvement over the existing free breathing (FB) SBRT. Free breathing
computed tomography (CT) scans in the treatment planning process, capture the
random position of a tumour and/or artefacts. Extensive literature has shown
the efficacy and safety of SBRT for peripheral and central tumors. A 2-year
local control range of 88% to 100% was noted by systematic reviews. 50 Gy in 5
fractions is often used for ultracentral tumors, whereas RTOG 0813 is a dose
escalation study of 5-fraction SBRT up to 12 Gy/fraction for central tumors.
The
challenge
The
respiratory motion is an important challenge for patients with moving targets
(6,7). The challenge frequently encountered during a radiation planning session
is how to design an appropriate plan for a moving target such as the lung. This
motion should be taken into consideration clinically to ensure that the target
receives the right dosage. This helps to minimize the toxicity associated with
irradiation of surrounding healthy tissue. Conventionally, larger margins are
used when creating a planning target volume from the clinical target volume.
Larger margins result in increased irradiated healthy tissue, possibly leading
to increased toxicity. The internal target volume defined during treatment
planning may not accurately cover the target range of motion during treatment
delivery. In free breathing CT scanning, respiratory organ motion can result in
significant geometrical distortion. The target may become longer or shorter due
to distortions along the axis of motion. The center of the imaged object may be
shifted by as much as the motion's amplitude in addition to shape distortion.
What
is 4DCT
A
tool used to measure the breathing motion is four-dimensional (4D) respiratory
correlated CT imaging (4DCT). It uses a gating mechanism. This gating can also
be used during treatment, such as when the deep inspiration breath-hold
technique is used, in which the radiation beam is only activated during
specific breathing cycle points (8, 9). Multiple CT images are produced by the
4D-CT, each of which shows the location and size of the tumor at a certain
breathing phase. Various available 4DCT methods practiced include slow CT,
prospective gated or breath hold CT, and retrospective 4DCT, each having their
own advantages. The tumor position with respect to the patient’s respiratory
cycle can be determined via the respiratory gating technique. The process involves
the use of an infrared tracking camera and a reflective marker placed on the
patient. The patient’s respiratory pattern and range of motion are displayed as
a waveform. Gating thresholds can be set along the waveform. This allows
patient-specific margins. Gating can be prospective or retrospective. For
retrospective image acquisition, continuous images are acquired. Retrospective
sorting can be done in either sinogram space (before reconstruction) or image
space (after reconstruction). Images can be sorted using either the breathing
phase or the amplitude phase.
To
develop a comfortable frequency and amplitude of breathing, it is crucial to
remember that the patient must get coaching. Compliance was defined as ability
to hold her breath for 20– 30 seconds. Understanding the movement of a tumor
within a patient can help customize treatment or even use tumor tracking or
gating technology to further limit normal tissue exposure and improve clinical
outcomes. The gross tumor volume (GTV) was defined as the lung tumor volume on
the basis of the planning 4D CT (with intravenous contrast) and fused PET
images. Tumor contouring is typically carried out during each breathing phase,
followed by the establishment of an internal target volume (ITV) that accounts
for the full movement cycle. Contouring was completed by multiphase Maximum
intensity projection (4D-MIP). The highest tumor velocity and tumor stability
is between 30-70% phases. Similarly, the internal target volume (ITV) was
defined using the 30% to 70% respiratory phase. A uniform 5 mm prescription
target volume (PTV) margin was expanded from the ITV. Planning uses the ECLIPSE
algorithm and the analytical anisotropic algorithm (AAA) for dose calculation.
Image guidance was based on CBCT during treatment.
Treatment
was prescribed for a total dose of 50 Gy in 5 fractions (BED10: 100 Gy) via
volumetric modulated arc therapy (VMAT). All critical structures were contoured
according to the RTOG 0915 guidelines. She was offered the adjuvant
capecitabine but did not comply. During surveillance imaging with PET/CT, there
was no sign of progression or distant failure, and the treated lesion responded
almost completely after 3 months beyond evidence of pneumonitis. Approximately
10% of patients have reported grade 3 or above toxicity, with fatal effects,
including hemorrhage, airway necrosis, and fistula formation. Our patient
developed grade 1 pneumonitis. She is being kept on regular follow-up and
advised to undergo lung physiotherapy and incentive spirometry.
Advantages
and disadvantages of 4DCT
4DCT
advantages: 1. It allows a potential decrease in the patient-specific ITV that
corresponds to a respiratory component.
2.
The 4DCT approach divides the CT data into distinct breathing stages, which
decreases or eliminates the irregularity.
3.
This approach benefits from free-breathing CT-based target delineation, which
assumes that the target is constant.
4.
Typically, the procedure involves defining the target volume for each phase,
the average intensity projection data sets, or the maximum intensity projection
(MIP).
5.
Compared with 3D-CT, 4D-CT improves target localization and minimizes motion
artifacts.
As a
result, during therapy, there is less radiation exposure to healthy tissue and
improved tumor coverage.
A
dosimetric study by Huang et al. assessed the accuracy of current stereotactic
body radiation therapy (SBRT) lung treatment planning methodologies for
irregular breathing patterns via MIP and AIP images generated from
four-dimensional computed tomography (4DCT). The study concluded that the
inaccuracy inherent in 4DCT MIP and AVG images could be mitigated by reducing
respiratory motion via volumetric image guidance (CBCT) or with abdominal
compressions. Average intensity projection (AIP) underestimates the ITV;
therefore, MIP is utilized for estimating size (10).
4DCT
Disadvantages
1.
Only a brief picture of the patient's breathing is taken; the entire breathing
pattern is not taken into consideration during treatment, particularly for
patients who have respiratory issues.
2.
In SBRT, 4DCT image artifacts are associated with poorer local control. With
erratic breathing and a comparatively short 4DCT acquisition period, it is
challenging to obtain enough data for artifact-free 4DCT reconstruction (11).
The
suggested method for overcoming the aforementioned drawbacks is the employment
of both 4D MRI and 5D CT, which allows for much longer acquisition periods and
mitigation strategies to reduce the severity of breathing disorders (12).
Second,
the efficacy of the system could be assessed by comprehensive 4DCT quality
assurance (QA).
Our
patient underwent Comprehensive QA prior delivery.
Advancements
The
CyberKnife System, a real-time robotic beam system, is the only radiotherapy
system that can maintain submillimeter precision during treatment delivery. It
has an integrated image guidance, automatic motion tracking, and retargeting
system to account for motion. It employs an orthogonal imaging system to
monitor movements during delivery with an optical camera placed above the
couch. In addition, diagnostic kV sources are fixed to the ceiling and floor
panel detectors, which further enhance its accuracy.
With
the advancement of technology, magnetic resonance imaging-guided radiotherapy
(MRIgRT) has become possible. It offers higher geometric accuracy and treatment
efficacy through online adaptation. The emphasis is now on the increased use of
artificial intelligence. With the development of wide field of view CT, 4DCT is
mostly used in the context of radiation therapy planning; nevertheless, it has
now opened up significant opportunities in the diagnostic sector.
Conclusion
Tumor movement is complex, with some showing superior
to inferior motion and others showing anterior to posterior motion. Tumor
displacement is dependent on the tumor site and location. The management of
respiratory motion is absolutely necessary. Our Study demonstrated superiority
of 4DCT over conventional techniques. Use of generic motion margins than custom
margins, help reduce normal tissue irradiation. For targets moving with
respiration and digestion, we suggest using 4DCT gated planning, as it is promising
due to its advantages and superior outcomes. The same was demonstrated in our
patient, with excellent results in surveillance image and resultant less tissue
toxicity.
Author
contribution
SA
and KG wrote
the main script, revised the script, conceptualized it, and prepared figures. SA
gathered resources.
Conflict
of interest
There
is no Conflicts of interest.
Funding
There
is no funding.
References
1. Nguyen DH, Truong PT, Walter CV: Limited M1
disease: a significant prognostic factor for stage IV breast cancer. Ann Surg
Oncol. 2012, 19:3028-34.
2. Dalenc F, Lusque A, De La Motte Rouge T: Impact of
lobular versus ductal histology on overall survival in metastatic breast
cancer: a French retrospective multicentre cohort study. Eur J Cancer. 2022,
164:70-9. 10.1016/j.ejca.2021.12.031
3, Cheruvu P, Metcalfe SK, Metcalfe J: Comparison of
outcomes in patients with stage III versus limited stage IV non-small cell lung
cancer. Radiat Oncol. 2011, 30:80.
4. Milano MT, Katz AW, Zhang H, Okunieff P:
Oligometastases treated with stereotactic body radiotherapy: long-term
follow-up of prospective study. Int J Radiat Oncol Biol Phys. 2012, 1:878-86.
5. Dahele M, Senan S: The role of stereotactic
ablative radiotherapy for early-stage and oligometastatic non small cell lung
cancer: evidence for changing paradigms. Cancer Res Treat. 2011, 43:75-82.
6. Boda-Heggemann J, Knopf AC, Simeonova-Chergou A,
Wertz H, Stieler F, Jahnke A, Jahnke L, Fleckenstein J, Vogel L, Arns A,
Blessing M, Wenz F, Lohr F. Deep Inspiration Breath Hold-Based Radiation
Therapy: A Clinical Review. Int J Radiat Oncol Biol Phys. 2016 Mar
1;94(3):478-92.
7. Kincaid RE Jr, Yorke ED, Goodman KA: Investigation
of gated cone-beam CT to reduce respiratory motion blurring. Med Phys. 2013,
40:041717.
8. Ford EC, Mageras GS, Yorke E:
Respiration-correlated spiral CT: a method of measuring respiratory-induced
anatomic motion for radiation treatment planning. Med Phys. 2003, 30:88-97.
9. Vedam SS, Keall PJ, Kini VR: Acquiring a
four-dimensional computed tomography dataset using an external respiratory
signal. Phys Med Biol. 2003, 7:45-62.
10. Use of maximum intensity projections (MIP) for
target volume generation in 4DCT scans for lung cancer Int J Radiat Oncol Biol
Phys. 2005; 63:253-260
11. Sentker T, Schmidt V, Ozga A-K, et al.: 4D CT
image arti facts affect local control in SBRT of lung and liver metastases.
Radiother Oncol.2020. 148:229-234.
12. Vergalasova I, Cai J: A modern review of the
uncertainties in volumetric imaging of respiratory-induced target motion in
lung radiotherapy. Med Phys.2020 47: e988-e1008. 10.1002/mp.1431.